[FS/2/2/2/2/4]
[[1]]
[Stamp of F Smith V.S. 12th Royal Lancers, dated 13.2.84]
Report on the recent outbreak of Anthrax among the horses of the Royal Artillery (I/3 and s/1) at the station of Bangalore during the month of December 1883
History
On the evening of the 5th December 1883 I returned from Mysore on duty and was met by Veterinary Surgeon Crows at the Railway Station who requested me to assist him in making a post mortem examination of an Elephant that had died that day and which he suspected had succumbed to Anthrax.
I proceeded to the place and the appearances presented by this beast on autopsy were identical with those seen in a horse which has suffered from the disease.
In all three elephants had died in two days. On returning late that evening we visited the Artillery lines as a horse had been reported “off feed” and on arrival we found three horses dead & one dying. There could be no doubt as to the nature of the malady. In S/1 Nos 39 & 42 had been admitted on the 4th Decr No 85 that day. In I/3 Nos 36 & 63 had been admitted at 6 pm that day.
On the following morning both batteries were moved out of their lines well to windward regular inspections of the healthy ordered and every possible means adopted to prevent contagion between the sick & healthy. On this day (6th Decr) the disease showed itself as a very virulent form no less than four horses of I/3 being admitted with it & two of S/1. Four died that day.
On the 7th Decr there was no sign of the disease abating seven horses were admitted “off feed” from I/3 and of these five died. Three were admitted from S/1 and these recovered. On this day I recommended I/3 to move ground which was done.
On the 8th Decr six horses were admitted again from I/3. Two of these died. S/1 furnished no cases this day.
On the 9th Decr There was a marked improvement in the health of both batteries, only two horses were reported “off feed” and both these recovered.
The 10th Decr saw the improvement continue, two more cases of “off feed” occured in I/3 these both recovered.
A whole week now elapsed without any cases presenting themselves when on the morning of 16th Decr a horse was admitted at 11:30 with
[[2]]
marked symptoms of the disease & died in a few hours.
The 17th & 18th passed in safety & on the 19th Decr the batteries were removed to Hebbel & left my charge.
It is important to notice that S/1 suffered but slightly, their burst on the first day was not fortunately followed up and practically no cases occurred in this battery after the 6th Decr. This I cannot account for, both batteries are placed as nearly as possible under identical conditions, both are in the open, their stables not 200 yards apart; the water supply is from the same source, their grain probably from the same place. In the matter of feeding there was however a vast difference. This will be dealt with hereafter.
Causes
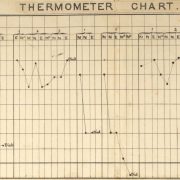
The weather in the early part of December was not in any way remarkable, here is a chart showing the direction of the wind and rainfall for the month:
[Table with data from 1-16 December 1883]
Now although there were no marked meteorological phenomena yet I think we may fairly consider among any probable causes the not improbable one of atmospheric influences. I do not mean by this that any
[[3]]
complex change was occurring in the chemical or other constituents of the atmosphere, for on this subject I cannot attempt to speculate but I do think it not improbable that the virus of the disease was present in the atmosphere and for the following cogent reason.
On the 4th & 5th Decr Anthrax occur simultaneously at the elephant lines, R.A lines, and among the horses of the 12th Royal Lancers I had three “off feed”. It would appear from this as if an Anthracogenic[sic] wave had passed over the station or at any rate this portion of it. I append a map showing the position of these several lines, the arrows shows the direction of the wind.
I am well aware that this speculation rather increases the difficulty of determining the cause than in assisting us in solving it, but the circumstance made an impression on me that no grass theory could remove for these elephants received no grass but were fed on cholum and sugar cane.
Whether an Anthracogenic[sic] wave really passed over might perhaps be determined by an examination of the records of cattle disease in the Province & neighboring taluks. I consider the [blank space] of importance because of the simultaneous outbreak of the disease in two distinct batteries, the cattle yard and not improbably the occurrence of three mild cases in a regiment of Cavalry. This is a very strong argument in favor of air poison, & very strong presumptive evidence against the grass. I would here explain that I partly recognize the influence that grass may have in introducing Anthrax into a regiment. but I do not think that in this case it suffices to account for the disease breaking out in so many different places within twelve hours of each other.
At the commencement of the outbreak we had no rise in the subsoil water but on the 13th, 14th & 16th Decr there was heavy rain. The significance of rain & Anthrax is marked. In a previous report I commented on this peculiarity.
The drinking water for both batteries as for the division (except the Native Cavalry) is from the Ulsoor Tank. the water trough of I/3 is by the side of the road exposed to any & every pollution. A year ago I pointed out the necessity of always having a sentry on the trough, and among the possible causes this is one to be considered.
Was this trough used by horses or cattle which had, or were suffering
[[4]]
from the disease? In my opinion it is not impossible but very improbable and I lay no particular stress on this point for the reason that S/1 suffered from the disease & the water trough of this battery is within the walls of their lines. The exposed position of the trough is the reason which prompts me to mention it.
With regard to feeding the two batteries were unlike. S/1 fed in the usual manner on Coolty and Grass, but the Officer Commanding I/3 with the object of curing skin disease amongst his horses, reduced the grass ration and gave cholum & ragi as well as the ordinary grass cutters grass. Was this cholum and ragi obtained from crops bordering on fields where Anthrax carcases[sic] lay or where diseased animals had been kept? It is singular that the elephants had been fed on choloum.
In one or two of the Post Mortem Exam: made I noticed large quantities of undigested cholum & ragi filling up the bowel, & where this had occurred the gut was intensely affected & almost gangrenous. This will prove the danger of giving to animals such coarse fodder during Anthrax time as it must destroy their slight chances of recovery.
Personally I place no faith in the cholum & ragi theory, but I mention the fact of the difference in the feeding owing to the disproportionate numbers of attacks in both batteries.
The grass of both batteries, as of that of all other mounted corps, is obtained anywhere, I speak advisedly, but to say that grass cutters go to a certain place to cut is an absurdity, some may or all would under European supervision, but the impossibility of the latter means that they get their bundles from the nearest place to their huts and I dont suppose that more than ten bundles in any one regiment are cut within a mile or more of each other. I do not think the grass theory explains this outbreak for reasons previously given, still in the present state of our knowledge, it is useless to speculate or point to one cause as being absolutely certain.
Symptoms and Post Mortem Appearances
There were more abdominal than [blank space] and throat cases. The proportions were [blank space]
The shortest time an animal lived from admission was three hours, the longest fourteen days. In one case the disease was localised in two or three feet of the Rectum which became enormously oedematous & protruded. The patient suffered acutely & nothing gave relief.
In a fatal throat case there was also a swelling in the near quarter.
[[5]]
This I have never seen before in the horse. The throat cases as usual lived longer (after a tube was inserted) than the abdominal ones, and the only patients which recovered, that undoubtedly had the disease, were mild throat cases, in neither of which it was found necessary to perform trachaeotomy.
I have previously submitted the post mortem description of a case which lasted fourteen days. The lessons one very instructive, & the case unusual. Beyond what I have mentioned there was nothing special in the symptoms & post-mortem appearances to distinguish it from others.
Treatment
I gave Iodine a fair bit in this outbreak. The dose was given was from half to one ounce of Iodine Pur: in a ball followed up by half an ounce every four hours. Intravenous injections were also given of the tincture. The results from Iodine are not very satisfactory, one undoubted case recovered that was treated with this agent. Hydrog: Bichlor was used in doses of ten grams twice a day, one undoubted case recovered which received this drug but the patient had also been treated with Carbolic Acid & the length of time the Hyd Bichlor was exhibited could not have been of any real value. It is singular that this patient refused to swallow any liquid medicine & I could waste to no more Carbolic Acid on him and so gave Hyd Bichlor in a ball. But he only received two or three doses when he showed such signs of returning health that I discontinued the drug so that practically I consider this case recovered without the use of medicine. Of the value of Carbolic Acid I am doubtful.
I administered preparations of Ammonia to most of the cases.
Progress
I am at a loss to know how the disease spreads after it breaks out. Is it by contagion or infection or both? I look upon the solution of this problem as being nearly equal in importance to the causes. I append a plan of the lines of I/3 showing the standings of each horse & of those attacked. It will be noticed some stood together or near each other but withal the cases were fairly well distributed through two double lines. Of course the probable means which suggest themselves to account for the spread of Anthrax are water troughs, nose bags (these I/3 did not use) and the virus being carried through the lines by horsekeepers. Still I am far from satisfied that these causes singularly or continued will fully account for its spread. Last year A troop 12th Royal Lancers suffered severely, these were under the same conditions as the other five troops of the regiment and yet these were not attacked. The water trough could have
[[6]]
spread the disease to the other troops but did not. In the same way S/I only lost 5 cases, yet these have infected the remainder of the battery either through the water trough or nose bags. I must really lean to poisoning through atmosphere, I mean infection.
But this subject is of immense importance and can only be settled by direct experiment. It is very singular in reference to the plan of the lines to note the number of cases which occurred among horses standing near each other or together. Yet such facts as these must not be taken as conclusive for there are many cases known where horses standing near diseased ones have remained unaffected & I know of two experiments made to determine this point both remaining negative. The last was made by V.S. Steel and among other things the same nose bag was used for both animals. Both Field Batteries all in open lines, there is no obstruction to a free current of air & the soil is clean. Sporadic Cases of Anthrax have occurred in the I/3 lines during the past year but from my enquiries no severe attack has shown itself in these lines for some years. It is different with S/I the year before last a battery of R.A which occupied these lines suffered very severely and I/3 at that time had not a single case.
The more one looks into these & other facts the more inexplicable these virulent outbreaks of Anthrax seem. What conditions determine sporadic cases & severe epizootics? What absolute proof have we that the disease is introduced into lines either by grass, water, air or soil? The whole matter is one of speculation.
Experimental Investigation We have made no experiments with the material which we perhaps justly condemn as the poison introducer or factor & I would urge that experimental investigation be carried out to show throw some light on the subject that it will throw light I am convinced.
To make myself clear I will take the following example: –
We strongly condemn the washing of grass, and we blame the grass in many cases as the means of introducing the disease. Now this is pure speculation, we have no single experiment to prove it. It could however be proved & that very simply. If dirty tank and nullah water will produce Anthrax why should not, say 12 horses cast for being incurable or worn out be watered entirely with water rather from these places. If within two months or more they all remained healthy after they have been watered from the worst places in Bangalore, we might
[[7]]
with safety reject this theory as being untenable and turn our attention to some other suspected points such as feeding our subjects on tank grass, or grass from flooded lands or from the graves of Anthrax cases or from grass which has undergone fermentation. Administer earth to them from suspected places such as they would receive as their grass, picket them on dung heaps or other places where decomposition of animal and vegetable matter is going on. If during these experiments Anthrax was produced observations could then be made as to the period of incubation, infection contagion & treatment. Altogether the enquiry would take twelve months but there is not a doubt much valuable & reliable information would be obtained regarding this disease at a very small cost to Government, & probably be the means of saving them thousands of rupees which are lost annually through its ravages.
This enquiry through a laborious one I should be perfectly willing to conduct without prejudice to my other duties.
Doubtful Cases
We have again in this outbreak to note the frequency of horses “off feed” all these cases have been entered in the Register as a “Simple Fever” & in the plan of the lines I have shown them as doubtful.
On scientific grounds I have been strongly opposed to recording these cases as Anthrax cured, but from the constancy with which they occur during the several outbreaks of the disease I have witnessed I am convinced that they are not the result of accident, but that they are full of significance. Can they be mild forms of the disease when the poison is endeavoring to obtain an entry into the system? Again we find ourselves speculating! Let this be settled by experimental investigation.
Research
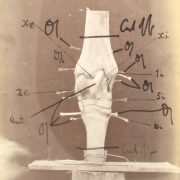
There was very little time for original research but the following observations on the microscopical appearances of the blood are of value. The blood was examined immediately it was taken from the body.
I/3 No 1
Examined on the first day of disease. No bacilla present, blood apparently normal. Case died next day.
[I/3 No] 10
Blood examined immediately after death, no bacilla red corpuscles, oily looking, seem deprived of much of their colour to an extent of outline. They collect as a structureless oily mass. Spores a few present.
[I/3 No] 18
Blood examined in the second day of disease, red cells oily as above, defective in outline, white cells numerous, serous fluid from
[[8]]
rectal protrusion, swarming with rods and spores. Patient died the following day.
I/3 No 22
Examined on the third day of disease. No bacilla or spores to be seen in the blood; blood cells shrunken stellata & granular. In the serum from swollen throat no sign of bacilla or spores. The blood of this patient was examined on the day of admission and nothing found in it.
Died on the fourth day of disease.
S/I [No] 48
Examined on the second day of disease. A throat case. Examined the blood from the tube & wound, found the cells had lost their outline, greasy, oily looking, and in clusters drew themselves out in long globules. No bacilla. This patient lived fourteen days, and after death I found no bacilla.
[S/I No] 104
Examined blood on the second day of disease no bacilli. Red corpuscles as before described, formed oily looking masses their definition lost & colour partially destroyed. This case a slight one recovered.
These observations are important. Bacilla were found in only once, & that from an acutely oedematous bowel. The changes to the red cells were very marked & I have attempted to draw them from memory. I am far from satisfied that this oily aggregation of red cells is constant in Anthrax, but I am assured of its presence in the above undoubted cases of the disease.
Statistics
The statistics of this outbreak are as follows:
I Battery 3rd Brig – Strength 110
Number of undoubted cases in proportion to the strength – 13 per cent
[Number of undoubted cases] that died ]in proportion to strength] – 12 [per cent]
[Number of] doubtful [cases in proportion to the strength] – 9 [per cent]
[Number of] undoubted cases that recovered in proportion to the attack – 7 [per cent]
Including all cases that recovered [in proportion to the attack] – 46 [per cent]
Number of deaths in proportion to the number of undoubted cases attacked – 93 [per cent]
S Battery 1st Brig – Strength 110
Number of undoubted cases in proportion to the strength – 4.5 per cent
[Number of undoubted cases] that died [in proportion to strength] – 3.5 [per cent]
[Number of] doubtful [cases in proportion to the strength] – 2.5 [per cent]
[Number of] undoubted cases that recovered in proportion to the attack – 20 [per cent]
Including all cases that recovered [in proportion to the attack] – 50 [per cent]
Number of deaths in proportion to the number of undoubted cases attacked – 80 [per cent]
[[9]]
In framing these statistics I have shown the recoveries & deaths of two ways. First as separate from doubtful cases & secondly in conjunction with them.
[Below text struck through and annotated ‘Cancelled’]
Conclusion
In conclusion I would beg to bring to your notice the manner in which I have been hampered in the performance of my duties by people who though entirely ignorant of the subject take upon themselves to pass strictures on my treatment. I spared neither time or trouble with these cases & brought the latest scientific views to bear on the epizooty. I therefore feel that justice has not been done me & entirely because I returned all doubtful cases as such and not as Anthrax Cured and also for the reason that my treatment was not that laid down for the guidance of Farriers in R.A. S.O published 13 years ago.
Vety Surgn
Bangalore
12th February 1884
To
The Inspecting Veterinary Surgeon
Madras Army.
[Transcription by Claudia Watts, KCL History, April 2019]